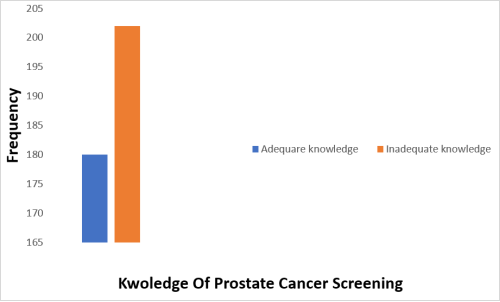
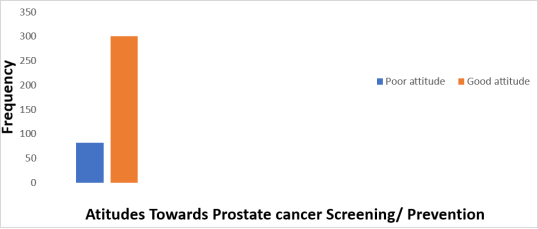
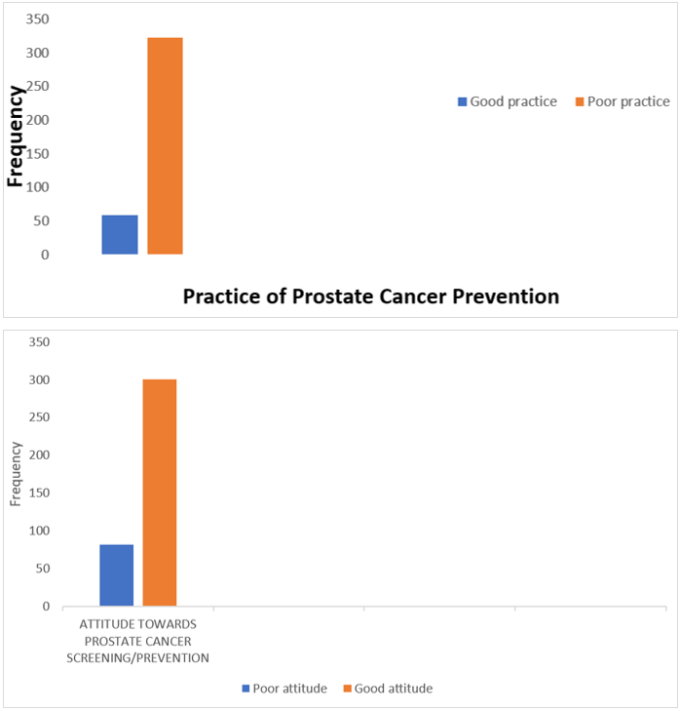
Prostate cancer is the second most common cancer globally and the fifth leading cause of cancer-related mortality in men, with approximately 1,200,000 new diagnoses and 359,000 deaths recorded in 2018. In Africa, it ranks as the most prevalent cancer, with 40,000 new cases and 28,000 cancer-related deaths annually. In Nigeria, it is the most common malignancy among men, accounting for 29.8% of all male cancers according to GLOBOCAN 2020 statistics. This study assessed the knowledge, attitudes, and practices related to prostate cancer prevention among men aged 20 to 80 years residing in the Okada community. A descriptive cross-sectional survey was conducted among 382 consenting male respondents. The self-administered questionnaire comprised four sections (A–D), addressing socio-demographic characteristics, knowledge of prostate cancer and screening, attitudes toward prostate cancer prevention, and prevention practices, respectively. The results revealed that 52.9% of respondents had inadequate knowledge of prostate cancer and screening. Although 67.8% had previously heard of prostate cancer, 78.5% demonstrated a positive attitude toward screening and prevention, while 84.6% exhibited poor prostate cancer prevention practices. The findings indicated that respondents with higher educational attainment possessed better knowledge of prostate cancer and screening than those with lower or no formal education. Younger men were more likely to express positive attitudes toward prostate cancer prevention. Furthermore, individuals with higher education levels were more likely to engage in effective prostate cancer prevention practices than those with limited or no formal education. Overall, respondents demonstrated inadequate knowledge of prostate cancer and screening, a generally positive attitude toward prevention, but poor preventive practices.
| Published in | American Journal of Internal Medicine (Volume 14, Issue 2) |
| DOI | 10.11648/j.ajim.20261402.12 |
| Page(s) | 23-34 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Prostate Cancer, Knowledge, Attitude, Practice
VARIABLES | ITEMS | FREQUENCY | PERCENTAGE (%) |
|---|---|---|---|
AGE | 20–30 | 72 | 18.8 |
31–40 | 130 | 34.0 | |
41–50 | 95 | 24.9 | |
51–60 | 48 | 12.6 | |
61–70 | 30 | 7.9 | |
71–80 | 7 | 1.8 | |
MARITAL STATUS | Single | 83 | 21.7 |
Married | 274 | 71.7 | |
Divorced | 6 | 1.6 | |
Widowed | 19 | 5.0 | |
RELIGION | Christian | 280 | 73.3 |
Muslim | 83 | 21.7 | |
Traditional | 17 | 4.5 | |
Non/Atheist | 2 | 0.5 | |
EDUCATIONAL LEVEL | Primary | 51 | 13.4 |
Secondary | 173 | 45.3 | |
Tertiary | 128 | 33.5 | |
No formal education | 30 | 7.9 | |
OCCUPATION | Civil servant | 77 | 20.2 |
Taxi driver | 88 | 23.0 | |
Businessman | 96 | 25.1 | |
Artisan/Handiwork | 72 | 18.8 | |
Other (Farming) | 49 | 12.8 | |
MONTHLY EARNINGS | Less than ₦10,000 | 7 | 1.8 |
₦10,000–30,000 | 65 | 17.0 | |
₦31,000–50,000 | 110 | 28.8 | |
₦51,000–70,000 | 94 | 24.6 | |
₦71,000–100,000 | 67 | 17.5 | |
Above ₦100,000 | 39 | 10.2 |
VARIABLES | ITEMS | FREQUENCY | PERCENTAGE (%) |
|---|---|---|---|
Ever heard of prostate cancer | Yes | 259 | 67.8 |
No | 123 | 32.2 | |
Source of information about prostate cancer | Friends | 48 | 12.6 |
Read about it | 69 | 18.1 | |
TV/Radio | 63 | 16.5 | |
Doctor | 27 | 7.1 | |
Nurse | 10 | 2.6 | |
Relative | 8 | 2.1 | |
Internet | 34 | 8.9 | |
Ever known anyone who had or died of prostate cancer? | Yes | 10 | 2.6 |
No | 254 | 66.5 | |
I don't know | 118 | 30.9 | |
Gender affected by prostate cancer | Men only | 162 | 42.4 |
Women only | 1 | 0.3 | |
Both men and women | 156 | 40.8 | |
I don't know | 63 | 16.5 | |
Risk factors for developing prostate cancer | Family history | 130 | 34.0 |
Alcohol intake | 60 | 15.7 | |
Age | 77 | 20.2 | |
Exercise | 24 | 6.3 | |
Diet | 40 | 10.3 | |
Smoking | 51 | 13.4 | |
Age group most likely to develop prostate cancer | Below 40 years | 19 | 5.0 |
40–50 | 20 | 5.2 | |
51–60 | 28 | 7.3 | |
61–70 | 17 | 4.5 | |
Above 70 years | 60 | 15.7 | |
I don't know | 238 | 62.3 | |
Cause of prostate cancer | Alcohol intake | 79 | 20.7 |
Multiple sexual partners | 135 | 35.3 | |
Family history | 53 | 13.9 | |
Use of sexual stimulants | 115 | 30.1 | |
Number of stages of prostate cancer development | 2 | 119 | 31.2 |
3 | 122 | 31.9 | |
4 | 49 | 12.8 | |
5 | 54 | 14.1 | |
6 | 17 | 4.5 | |
Other (7, 8, 10) | 21 | 5.5 | |
Anyone can develop prostate cancer | Yes | 54 | 14.1 |
No | 114 | 29.8 | |
I don't know | 214 | 56.1 | |
Symptoms of prostate cancer | Excessive urination at night | 76 | 19.9 |
Headache | 22 | 5.8 | |
Blood in urine | 56 | 14.7 | |
High temperature | 44 | 11.5 | |
Bone pain | 60 | 15.7 | |
Painful sex | 51 | 13.4 | |
Loss of sex drive | 29 | 9.9 | |
Infertility | 38 | 7.6 | |
Cough | 6 | 1.6 | |
Prostate cancer can be prevented | Yes | 240 | 62.8 |
No | 50 | 13.1 | |
I don't know | 92 | 24.1 | |
If yes, how can it be prevented? | Genital hygiene | 84 | 22.0 |
Regular screening | 64 | 16.8 | |
Condom use | 13 | 3.4 | |
Appropriate diet | 47 | 12.4 | |
Avoiding multiple partners | 41 | 12.3 | |
Other (avoid smoking) | 3 | 0.8 | |
Prostate cancer is curable | Yes | 174 | 45.5 |
No | 50 | 13.1 | |
I don't know | 158 | 41.4 | |
At what stage can it be cured? | Early stage | 102 | 26.7 |
Anytime treatment begins | 25 | 6.5 | |
Late stage | 6 | 1.6 | |
I don't know | 122 | 31.9 | |
Do you know any method used in treating prostate cancer? | Yes | 228 | 59.7 |
No | 154 | 40.3 | |
If yes, which method do you know? | Radiotherapy only | 1 | 0.3 |
Surgery only | 68 | 17.8 | |
Drugs only | 101 | 26.4 | |
Radiotherapy and surgery only | 4 | 1.0 | |
Radiotherapy and drugs only | 9 | 2.4 | |
Surgery and drugs only | 40 | 10.5 | |
Surgery, drugs, and radiotherapy | 5 | 1.3 | |
Herbal/traditional medicine | 1 | 0.3 | |
Have you ever heard about prostate cancer screening/testing? | Yes | 124 | 32.5 |
No | 232 | 60.7 | |
I don't know | 26 | 6.8 | |
Source of information (if yes) | Hospital | 39 | 10.2 |
Pharmacy | 10 | 2.6 | |
Friends | 8 | 2.1 | |
Relative | 7 | 1.8 | |
Radio/TV | 30 | 7.9 | |
Newspaper/book/magazine | 22 | 5.8 | |
Other (internet) | 12 | 3.1 | |
How often should one undergo prostate cancer screening? | Yearly | 59 | 15.4 |
Every two years | 21 | 5.5 | |
Every three years | 18 | 4.7 | |
I don't know | 284 | 74.4 |
VARIABLES | ITEMS | FREQUENCY | PERCENTAGE (%) |
|---|---|---|---|
Prostate cancer screening is beneficial | Yes | 368 | 96.3 |
No | 14 | 3.7 | |
Going for prostate cancer screening is a waste of time | Yes | 19 | 5.0 |
No | 363 | 95.0 | |
Screening for prostate cancer has side effects | Yes | 11 | 2.9 |
No | 168 | 44.0 | |
I don't know | 203 | 53.1 | |
Prostate cancer screening is the only means to diagnose prostate cancer | Yes | 33 | 8.6 |
No | 34 | 8.9 | |
I don't know | 315 | 82.5 | |
It is important to get screened to prevent prostate cancer | Strongly agree | 220 | 57.6 |
Agree | 142 | 37.2 | |
Disagree | 16 | 4.2 | |
Strongly disagree | 4 | 1.0 | |
Prostate cancer screening is embarrassing to me | Strongly agree | 10 | 2.6 |
Agree | 27 | 7.1 | |
Disagree | 146 | 38.2 | |
Strongly disagree | 199 | 52.1 | |
What do you think prevents people from getting screened? | Lack of knowledge | 242 | 63.4 |
Fear of the unknown | 73 | 19.1 | |
Deliberate avoidance of testing | 50 | 13.1 | |
Religious beliefs | 17 | 4.5 | |
I believe there is nothing one can do to prevent prostate cancer | Strongly agree | 12 | 3.1 |
Agree | 24 | 6.3 | |
Disagree | 215 | 56.3 | |
Strongly disagree | 131 | 34.3 | |
Would you present yourself for prostate cancer screening if given the opportunity? | Yes | 325 | 85.1 |
No | 42 | 11.0 | |
I don't know | 15 | 3.9 |
VARIABLES | ITEMS | FREQUENCY | PERCENTAGE (%) |
|---|---|---|---|
Has any physician advised you to screen for prostate cancer? | Yes | 53 | 13.9 |
No | 315 | 82.5 | |
I don't know | 14 | 3.7 | |
Have you ever been screened for prostate cancer? | Yes | 8 | 2.1 |
No | 370 | 96.9 | |
I don't know | 4 | 1.0 | |
If yes, which method was used? | Prostate-specific antigen (PSA) | 2 | 0.5 |
Digital rectal examination (DRE) | 1 | 0.3 | |
Biopsy | 3 | 0.8 | |
I don't know | 2 | 0.5 | |
What was the outcome? | Positive | — | — |
Negative | 8 | 1.7 | |
Do you intend to get screened in the near future? | Yes | 311 | 81.4 |
No | 71 | 18.6 | |
When did you last undergo prostate cancer screening? | Last month | 1 | 0.3 |
3 months ago | — | — | |
6 months ago | — | — | |
1 year ago | — | — | |
Never | 375 | 98.2 | |
Other (3–5 years ago) | 6 | 1.6 |
KAP | Knowledge, Attitude, and Practice |
PSA | Prostate-Specific Antigen |
DRE | Digital Rectal Examination |
NPC | National Population Commission |
SPSS | Statistical Package for Social Sciences |
GLOBOCAN | Global Cancer Observatory/Global Cancer Statistics |
NGO | Non-Governmental Organization |
CI | Confidence Interval |
OR | Odds Ratio |
WHO | World Health Organization |
| [1] | Bray, F., Ferlay, J., Soerjomataram, I., Siegel, R. L., Torre, L. A., & Jemal, A. (2018). Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: A Cancer Journal for Clinicians, 68(6), 394–424. |
| [2] | Ferlay, J., Shin, H. R., & Bray, F. (2011). Estimates of worldwide burden of cancer: GLOBOCAN 2008. International Journal of Cancer, 127, 2893–2917. |
| [3] | Desousa, A., Sonavane, S., & Mehta, J. (2012). Psychological aspects of prostate cancer. Prostate Cancer and Prostatic Diseases, 15(2), 120–127. |
| [4] | American Cancer Society. (2019). Cancer facts and Figures, 2019. Atlanta, GA: American Cancer Society. |
| [5] | Nakandi, H., Kirabo, M., Semugabo, C., Kittengo, A., Kitayimbwa, P., Kalungi, S., & Maena, J. (2015). Knowledge, attitudes, and practices of Ugandan men regarding prostate cancer. African Journal of Urology, 19, 165–170. |
| [6] | Deibert, C. M., Maliski, S., & Kwan, L. (2007). Prostate cancer knowledge among low-income minority men. Journal of Urology, 177, 1851–1855. |
| [7] | Ojewola, R. W., Oridota, E. S., & Olanrewaju, S. B. (2017). Knowledge, attitudes, and screening practices regarding prostatic diseases among men older than 40 years: A population-based study in Southwest Nigeria. Pan African Medical Journal, 27, 151. |
| [8] | Kanungo, S., Bhowmik, K., Mahapatra, T., Mahapatra, S., Bhadra, U. K., & Sarkar, K. (2015). Perceived morbidity, healthcare-seeking behavior and determinants in a poor-resource setting: Observations from India. PLoS ONE, 10(5), e0125865. |
| [9] | Oladimeji, O., Bidemi, Y. O., Olufisayo, J. A., & Sola, A. O. (2010). Prostate cancer awareness, knowledge, and screening practices among older men in Oyo State, Nigeria. International Quarterly of Community Health Education. |
| [10] | Olapade-Olaopa, E. O., Obamuyide, H. A., & Yisa, G. T. (2008). Management of advanced prostate cancer in Africa. Canadian Journal of Urology, 15, 3890–3898. |
| [11] | Deborah, O. A., Anyachebelu, O. C., Azubuike, E. A., & Abdulmuminu, I. (2018). Knowledge, attitudes, and perception of prostate cancer among male outpatients of a tertiary care hospital in south-east Nigeria. Journal of Applied Pharmaceutical Science, 8(11), 064–068. |
| [12] | Mohammed-Faez-Baobaid, Mohammed-A.-Abdalqader, Hasanain-Faisal-Ghazi, Hesham-Shebl, & Haitham-Assem-Abdalrazak. (2020). The study of knowledge, attitude, and practice of prostate cancer prevention and its relationship with socio-demographic characteristics among men at Ppr Lembah Subang 1, Selangor. Malaysian Journal of Medicine and Health Sciences, 46–51. |
| [13] | Sakala, G., Kasongo, N., & Mwanakasale, V. (2020). Assessment of knowledge, practice, and attitude towards prostate cancer screening among male patients aged 40 years and above at Kitwe Teaching Hospital, Zambia. African Journal of Urology, 26(1). |
| [14] | Oranusi, C. K., Mbieri, U. T., Oranusi, I. O., & Nwofor, A. M. E. (2012). Prostate cancer awareness and screening among male public servants in Anambra State, Nigeria. African Journal of Urology, 18, 72–74. |
| [15] | Chamie, K., Williams, S. B., & Hu, J. C. (2015). Population-based assessment of determining treatments for prostate cancer. JAMA Oncology, 1(1), 60–67. |
| [16] | De Paiva, E. P., Salvador da Motta, M. C., & Griep, R. H. (2010). Knowledge, attitudes, and practices regarding the detection of prostate cancer. Acta Paulista de Enfermagem, 23(1), 88–93. |
| [17] | Morlando, M., Pelullo, C. P., & Di Giuseppe, G. (2017). Prostate cancer screening: Knowledge, attitudes, and practices in a sample of men in Italy. A survey. PLoS ONE. |
APA Style
Isaiah, O. O. (2026). Assessment of Knowledge, Attitude, and Practice of Prostate Cancer Prevention Among Male Residents. American Journal of Internal Medicine, 14(2), 23-34. https://doi.org/10.11648/j.ajim.20261402.12
ACS Style
Isaiah, O. O. Assessment of Knowledge, Attitude, and Practice of Prostate Cancer Prevention Among Male Residents. Am. J. Intern. Med. 2026, 14(2), 23-34. doi: 10.11648/j.ajim.20261402.12
@article{10.11648/j.ajim.20261402.12,
author = {Ogunsina Olabode Isaiah},
title = {Assessment of Knowledge, Attitude, and Practice of Prostate Cancer Prevention Among Male Residents},
journal = {American Journal of Internal Medicine},
volume = {14},
number = {2},
pages = {23-34},
doi = {10.11648/j.ajim.20261402.12},
url = {https://doi.org/10.11648/j.ajim.20261402.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.ajim.20261402.12},
abstract = {Prostate cancer is the second most common cancer globally and the fifth leading cause of cancer-related mortality in men, with approximately 1,200,000 new diagnoses and 359,000 deaths recorded in 2018. In Africa, it ranks as the most prevalent cancer, with 40,000 new cases and 28,000 cancer-related deaths annually. In Nigeria, it is the most common malignancy among men, accounting for 29.8% of all male cancers according to GLOBOCAN 2020 statistics. This study assessed the knowledge, attitudes, and practices related to prostate cancer prevention among men aged 20 to 80 years residing in the Okada community. A descriptive cross-sectional survey was conducted among 382 consenting male respondents. The self-administered questionnaire comprised four sections (A–D), addressing socio-demographic characteristics, knowledge of prostate cancer and screening, attitudes toward prostate cancer prevention, and prevention practices, respectively. The results revealed that 52.9% of respondents had inadequate knowledge of prostate cancer and screening. Although 67.8% had previously heard of prostate cancer, 78.5% demonstrated a positive attitude toward screening and prevention, while 84.6% exhibited poor prostate cancer prevention practices. The findings indicated that respondents with higher educational attainment possessed better knowledge of prostate cancer and screening than those with lower or no formal education. Younger men were more likely to express positive attitudes toward prostate cancer prevention. Furthermore, individuals with higher education levels were more likely to engage in effective prostate cancer prevention practices than those with limited or no formal education. Overall, respondents demonstrated inadequate knowledge of prostate cancer and screening, a generally positive attitude toward prevention, but poor preventive practices.},
year = {2026}
}
TY - JOUR T1 - Assessment of Knowledge, Attitude, and Practice of Prostate Cancer Prevention Among Male Residents AU - Ogunsina Olabode Isaiah Y1 - 2026/06/30 PY - 2026 N1 - https://doi.org/10.11648/j.ajim.20261402.12 DO - 10.11648/j.ajim.20261402.12 T2 - American Journal of Internal Medicine JF - American Journal of Internal Medicine JO - American Journal of Internal Medicine SP - 23 EP - 34 PB - Science Publishing Group SN - 2330-4324 UR - https://doi.org/10.11648/j.ajim.20261402.12 AB - Prostate cancer is the second most common cancer globally and the fifth leading cause of cancer-related mortality in men, with approximately 1,200,000 new diagnoses and 359,000 deaths recorded in 2018. In Africa, it ranks as the most prevalent cancer, with 40,000 new cases and 28,000 cancer-related deaths annually. In Nigeria, it is the most common malignancy among men, accounting for 29.8% of all male cancers according to GLOBOCAN 2020 statistics. This study assessed the knowledge, attitudes, and practices related to prostate cancer prevention among men aged 20 to 80 years residing in the Okada community. A descriptive cross-sectional survey was conducted among 382 consenting male respondents. The self-administered questionnaire comprised four sections (A–D), addressing socio-demographic characteristics, knowledge of prostate cancer and screening, attitudes toward prostate cancer prevention, and prevention practices, respectively. The results revealed that 52.9% of respondents had inadequate knowledge of prostate cancer and screening. Although 67.8% had previously heard of prostate cancer, 78.5% demonstrated a positive attitude toward screening and prevention, while 84.6% exhibited poor prostate cancer prevention practices. The findings indicated that respondents with higher educational attainment possessed better knowledge of prostate cancer and screening than those with lower or no formal education. Younger men were more likely to express positive attitudes toward prostate cancer prevention. Furthermore, individuals with higher education levels were more likely to engage in effective prostate cancer prevention practices than those with limited or no formal education. Overall, respondents demonstrated inadequate knowledge of prostate cancer and screening, a generally positive attitude toward prevention, but poor preventive practices. VL - 14 IS - 2 ER -
Department of Public Health, Olusegun Agagu University of Science and Technology, Okitipupa, Nigeria;Department of Pharmacy, Igbinedion University, Okada, Nigeria;Majestic Vistal Pharmaceutical Ltd., Akure, Nigeria
Information